When researchers test a new medicine or even a new program design, they often devise a study comparing results between a treatment group and a control group. People in the control group receive no treatment, and forgo any benefits if it is proven to work and avoid any side effects if proven harmful.
A trial is going on regarding healthcare in this country, and right now Oklahoma has put itself in the control group. In this case, being in the control group may not be in our state’s best interest. However, it will provide useful comparisons between our state and states that chose to expand Medicaid.
 In 2012, in the same decision where the Supreme Court ruled the bulk of the Affordable Care Act (ACA) was constitutional, the court also ruled that the federal government could not force the states to accept the Medicaid expansion. The Medicaid expansion was intended to provide healthcare coverage for Americans whose income fell below 133% of the poverty level.
In 2012, in the same decision where the Supreme Court ruled the bulk of the Affordable Care Act (ACA) was constitutional, the court also ruled that the federal government could not force the states to accept the Medicaid expansion. The Medicaid expansion was intended to provide healthcare coverage for Americans whose income fell below 133% of the poverty level.
While the court ruled the federal government could not force states to expand Medicaid eligibility, it did keep the option alive for states willing to accept federal money for the expansion. In essence, the final decision on expanding Medicaid fell to the individual states.
However, declining the expansion does not leave states in the same situation they were in before the ACA was passed. In 2014, all states will begin to see a decline in the Disproportionate Share Hospital (DSH) payments the federal government grants to states to fund care for indigent patients.
States used DSH payments to help hospitals deal with unpaid medical bills, and DSH payments are decreasing because Medicaid was supposed to fill the gap. So it is important to understand that declining additional Medicaid funds leaves many hospitals at a financial disadvantage.
According to the Kaiser Family Foundation, 27 states (including D.C.) have decided to expand Medicaid, 3 states are still debating the issue, and 21 states have turned down the expansion. In at least 21 states, there is now a group of people who fall into the “Medicaid Gap,” because they make too much money to qualify for traditional Medicaid but not enough money to qualify for a federal subsidy to buy private insurance. (Incomes between 100% and 400% of the federal poverty guidelines qualify for a subsidy, or tax credit, to buy insurance.)
The magnitude of the “Medicaid Gap” can be seen in early predictions. The Robert Wood Johnson Foundation and Urban Institute studied 14 “large and diverse” cities and predicts that by 2016 the 7 cities located in states expanding Medicaid will see a 57% drop, on average, in the number of uninsured. The 7 cities in states that declined the expansion will only decrease the number of uninsured by an average of 30%.

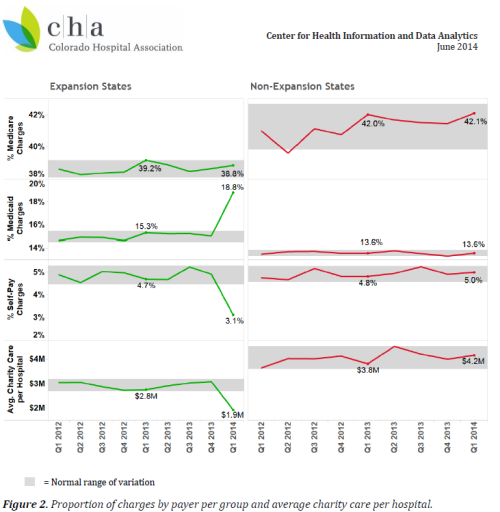
This lack of insurance has a financial impact on hospitals. Because Oklahoma is not expanding Medicaid, our hospitals are not seeing the decline in self-pay and charity care from which hospitals in other states are already benefiting, according to a report by the Colorado Health Association (CHA).
The CHA study included 465 hospitals in 30 states, 15 of which expanded Medicaid and 15 of which did not, including Oklahoma. Starting in the first quarter of 2014, hospitals in states that expanded Medicaid saw an increase in Medicaid charges, while simultaneously seeing a drop in self-pay and charity care. The CHA noted the changes were not only distinct, but substantial.
Meanwhile, the Oklahoma Health Care Authority (OHCA), which administers the state’s Medicaid program, has a $225 million budget shortfall to resolve. In addition to slashing payment rates to doctors and hospitals, the OHCA is also considering raising co-payments to the federal maximum.
Increasing co-payments is not sound policy, however. David Blatt, writing in an opinion piece for the Tulsa World, cites studies that show low-income Medicaid recipients often ration their own care because they cannot afford higher co-pays. One study tied higher co-pays to an 88% increase in the emergency room usage, which ultimately leads to higher costs. Blatt points out that rather than cutting benefits, Oklahoma could have expanded Medicaid.
So far, Oklahoma is not seeing any verifiable advantage from refusing the Medicaid expansion, while other states, such as Colorado, are already reporting benefits. In June, Mercy hospital system announced the layoff of up to 300 employees across 4 states, including Oklahoma. They cite the lack of Medicaid expansion as a reason for the cut backs.
The OK Policy Blog points out that community health centers in Oklahoma, who treat underserved populations regardless of their ability to pay, are struggling as well. The state’s uncompensated care fund is one of many resources community health centers draw from to recoup the financial loss when patients are unable to pay, and it ran dry in December of 2013. Some of the financial burden on these centers could have been eased by expanding Medicaid.
There is a real world cost to declining funds to expand Medicaid. There are also real world benefits to expanding it. As the Center on Budget and Policy Priorities wrote in April, Medicaid has proven to be efficient, giving states flexibility to design their own programs, providing beneficiaries with better access to care compared to the uninsured, and doing more to encourage work and increased income than the traditional program.
Oklahoma could do more to improve the health of the thousands of citizens without health insurance. However, if we decide to voluntary remain in the control group, the coming years may easily prove to be expensive for the citizens who cannot afford health care and the hospitals who face unpaid bills without federal funding to mitigate the loss.
- Last December, OK Policy Blog wrote about the different approaches being taken by Kentucky and Oklahoma in relation to the Affordable Care Act.
- The New York Times published a piece in early June, “In Texarkana, Uninsured and on the Wrong Side of a State Line,” about how the health outcomes of Arkansas and Texas citizens could be vastly different because of their approaches to Medicaid expansion.


Leave a comment